The Death of the Annual Report: Why Static Registries Fail Modern Cardiac Care
Static registries were built for a different era. Modern cardiac care demands living infrastructure that updates continuously and supports decisions at the point of care.
By Robert Kelly, Founder & CEO, Heart Rhythm International
Cardiac care is no longer a single event. It is a lifelong journey. It is time our data infrastructure reflected that.
Most health registries were built for a different era. They were designed to answer questions months, sometimes years, later. How many devices were implanted? What was the complication rate? Which hospital did what volume?
That type of retrospective reporting still has value, but it is no longer sufficient for modern cardiac care.
Today, cardiac services manage patients who live longer, carry more complex devices, and move frequently between hospitals, systems, and care settings. Follow-up is continuous, not episodic. Decisions are time-sensitive. Governance expectations are higher.
In that environment, a registry that updates quarterly is simply not fit for purpose. A static registry might work for an annual report. It does not work for real-world care.
Cardiac care is no longer an event
Cardiac rhythm management is not a single procedure followed by closure. It is a long-term clinical journey.
A patient may have an implant today, an MRI query next year, a lead issue in year five, and a generator replacement in year eight. Their care may span public and private hospitals, different consultants, and multiple clinical teams.
Over time, device details, leads, procedures, follow-ups, alerts, and outcomes become scattered across systems. When data fragments, clinicians lose time. Services lose visibility. Risk increases.
A snapshot view of a patient is no longer good enough.
Why static registries struggle
Static registries tend to fail in three predictable ways.
They are designed for reporting, not care. Most registries are optimised to produce tables, extracts, and dashboards for oversight and compliance. The data model reflects what is needed to fill in forms, not what clinicians need to see at the point of care. Clinicians do not need a registry to tell them what was true six months ago. They need to know what is true now.
They treat device patients as episodes, not populations. Many registries capture the implant event and little more. But rhythm patients are a population that requires ongoing management. Remote transmissions, alerts, complications, recalls, replacements, and longitudinal trends matter far more than a single procedure record. Static systems struggle here because they were never built to represent time, change, and continuity.
They cannot keep pace with governance and scale. Expectations around device traceability, auditability, and post-market surveillance have increased significantly, particularly in Europe. Compliance is no longer an administrative afterthought. It is operational. When systems cannot answer basic questions quickly and confidently, teams resort to workarounds: spreadsheets, scanned PDFs, manual lookups, phone calls between departments, and reliance on "institutional memory." None of this scales, and all of it introduces risk.
What modern cardiac services actually need
Modern cardiac care requires a different type of registry, one that behaves less like a static database and more like clinical infrastructure.
At a minimum, a modern registry needs to do five things well.
Update continuously. Data needs to be captured as part of routine workflow, not retrospectively. That is when it is most accurate and least burdensome.
Connect the full device story. Implant details are only the beginning. A registry must link devices, leads, procedures, follow-ups, outcomes, replacements, and changes over time into a single longitudinal record.
Support decisions at the point of care. The system should reduce cognitive load, not add to it. Clinicians should be able to find trusted information quickly and move on.
Deliver traceability by default. Audit logs, structured data capture, consistent identifiers, and device-level traceability must be built in, not layered on afterwards.
Enable the next layer of care. Predictive analytics and early warning tools are only possible if the underlying data is timely, structured, and longitudinal.
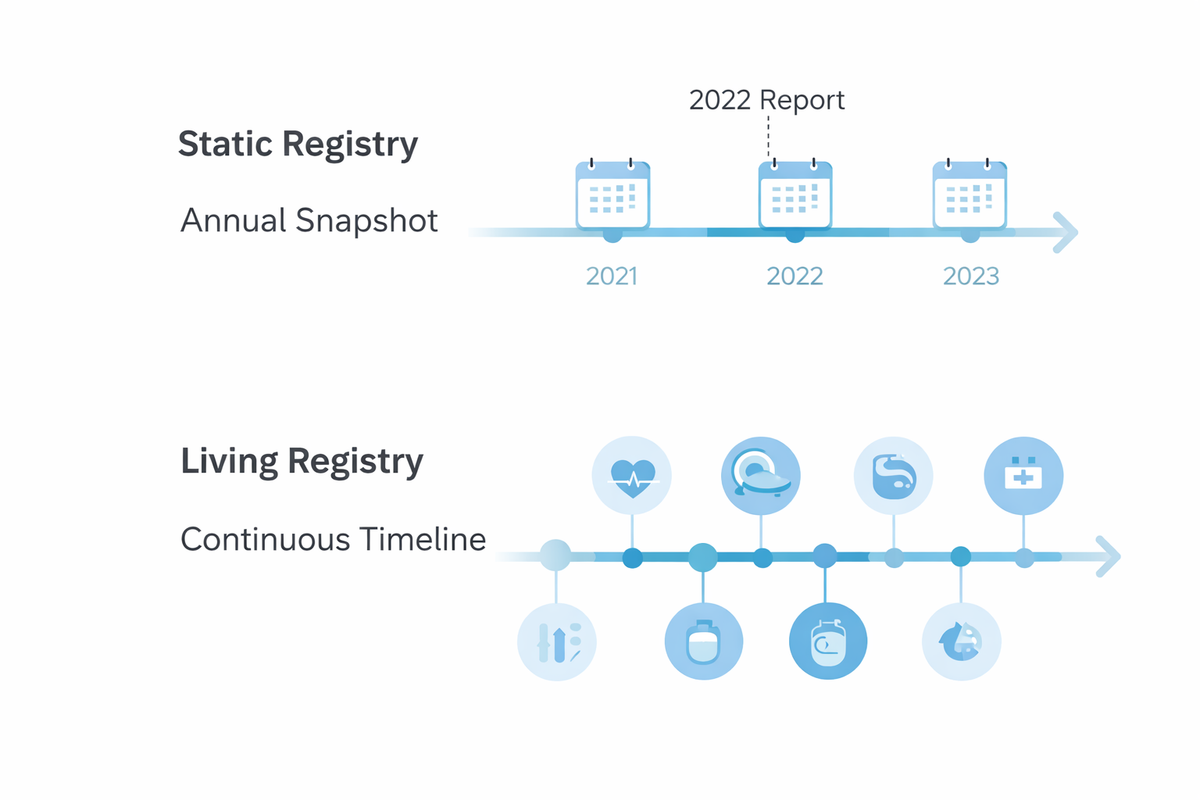
From registry as report to registry as infrastructure
This is the real shift that needs to happen.
A static registry is something you query after the fact. A living registry is something you operate every day. It sits quietly in the background, ensuring that accurate, up-to-date information is available across hospitals, teams, and years of care.
That shift changes everything. Retrospective reporting becomes real-time readiness. Administrative burden becomes clinical utility. Fragmented records become a single longitudinal view. Searching for data becomes trusting it.
Why this matters in practice
Consider the types of questions rhythm services deal with every week. What device does this patient have? Is the lead MRI conditional? Has the device been replaced? What is the exact model and serial number? Who implanted it, and where?
In a static registry model, these questions generate friction, delays, and extra work. In a living registry model, they are answered in seconds.
That difference is not academic. It affects patient safety, service efficiency, and clinician confidence.
A brief note on HRI
For over 17 years, Heart Rhythm International has been building national cardiac infrastructure designed to function as a living registry rather than a static reporting database.
We did not build a reporting tool. We built living clinical infrastructure that supports day-to-day cardiac care while meeting national governance requirements.
The aim has always been straightforward: accurate, longitudinal device records that fit naturally into hospital workflows and stand up to scrutiny over time.
Closing thought
Static registries are not failing because the idea of registries is wrong. They are failing because the operating model has not kept pace with how cardiac care is actually delivered.
Care is continuous. Data is longitudinal. Governance expectations are higher.
A registry that only exists to be reported on is no longer enough.
A registry needs to live.